Introduction
According to the National Institutes of Health (2024), the rs429358 variant is the strongest genetic risk factor for late-onset Alzheimer's disease, affecting approximately one-quarter of the global population. This single DNA variant determines whether you carry the APOE ε4 allele—an allele associated with significantly elevated Alzheimer's risk through impaired cholesterol and amyloid-beta processing in your brain.
Understanding rs429358 isn't about predicting your future: roughly half of those carrying two copies never develop Alzheimer's. Instead, knowing your status enables evidence-based prevention strategies that can substantially reduce risk. This comprehensive guide explains what rs429358 means, how it influences Alzheimer's risk, and what you can do about it if you carry this variant.
In this article, you'll discover how genetic risk works, explore all APOE combinations and their implications, learn personalized prevention strategies supported by neuroscience research, and find answers to common questions about rs429358 testing and management.
What is rs429358? Understanding the APOE ε4 Variant
rs429358 is a specific DNA variant (SNP—single nucleotide polymorphism) located on chromosome 19 within the APOE gene, which encodes apolipoprotein E, a protein responsible for transporting cholesterol and lipids throughout your brain. This single position in your DNA determines whether you inherit the APOE ε4 allele, the variant most strongly associated with increased Alzheimer's disease risk. At rs429358, the T allele indicates APOE ε4 status, while the C allele indicates APOE ε3 (the neutral variant).
Molecular Mechanisms: How APOE ε4 Damages the Brain
The mechanism explaining why APOE ε4 increases Alzheimer's risk involves several interconnected biological pathways. The ε4 variant impairs clearance of amyloid-beta proteins—sticky fragments that accumulate into plaques damaging nerve-to-nerve communication in the brain. Unlike APOE ε3, which moderately binds amyloid-beta, the ε4 variant binds avidly but forms stable complexes resistant to clearing, allowing plaques to accumulate.
This variant also drives neuroinflammation, an excessive immune response within the brain that damages neurons and their connections. ε4 carriers show reduced integrity of the blood-brain barrier—the protective filter regulating what enters your brain—making it more permeable to harmful substances and pathogens. Additionally, APOE ε4 impairs cholesterol metabolism in the brain, critical for myelin (the insulation coating nerve fibers) and cell membrane structure. Synaptic plasticity—your brain's ability to form new connections and adapt—is reduced in ε4 carriers, and the glymphatic system that clears metabolic waste during sleep functions less efficiently.
APOE ε4 in Evolutionary Context
APOE ε4 appears to be an evolutionarily recent mutation that arose relatively recently in human history. The ε3 variant represents the ancestral form, while ε2 and ε4 emerged through later genetic changes. Scientists theorize that ε4 provided advantages in certain historical environments (enhanced lipid transport, memory function in youth) but now imposes costs in modern aging populations where we live decades longer than our ancestors evolved to survive.
Understanding this context—that genetic risk isn't moral failure but rather evolutionary mismatch—helps remove stigma and focuses your attention on what you can control: modifiable risk factors that can offset genetic predisposition.
rs429358 and Alzheimer's Disease Risk: What the Science Shows
Alzheimer's risk increases sharply with rs429358 status and APOE genotype, but genetic risk is never absolute. The relationship is dose-dependent: more ε4 alleles mean higher probability, but other factors substantially modify this baseline risk.
Dose-Dependent Risk Stratification
| APOE Genotype | Prevalence | Lifetime Risk | Typical Age of Onset | Key Facts |
|---|---|---|---|---|
| ε3/ε3 (CC) | 60% | 10-15% | 80s+ | Baseline reference; neutral genotype |
| ε3/ε4 (CT) | 20-25% | 25-30% | 70s-75 | 3-4 fold increase; one ε4 allele |
| ε4/ε4 (TT) | 2-3% | 50-60% | 60s-70 | 8-12 fold increase; two ε4 alleles |
Research from Mayo Clinic confirms that ε3/ε3 carriers (the most common genotype) experience approximately 10-15% lifetime Alzheimer's risk, serving as the reference point. Those inheriting one ε4 allele (ε3/ε4, affecting 20-25% of people) face roughly 25-30% lifetime risk—a 3-4 fold increase. Those carrying two ε4 alleles (ε4/ε4, only 2-3% of the population) experience the highest risk at 50-60% lifetime probability.
Critically, these percentages represent population-level probabilities, not personal destiny. Many individuals with high-risk genotypes never develop cognitive decline, suggesting that genetic predisposition interacts dynamically with lifestyle, other genetic variants, education level, cardiovascular health, and environmental factors.
Gender and Sex Hormone Effects
Female APOE ε4 carriers consistently show higher Alzheimer's risk compared to males with identical genotypes—an important discovery from Alzheimer's Research UK (2024) and Stanford research. This sex difference emerges partly because estrogen, naturally produced pre-menopause, provides protective effects against ε4-related brain changes. Estrogen enhances clearance of amyloid-beta, maintains blood-brain barrier integrity, and suppresses neuroinflammation.
The post-menopausal period becomes a critical window for female ε4 carriers. The sharp decline in estrogen production after menopause accelerates cognitive aging in these women specifically. Some research suggests that hormone replacement therapy might offer modest cognitive benefits for female ε4 carriers, though this remains controversial and requires discussion with healthcare providers considering individual risks and benefits.
Female-specific prevention strategies become especially important: particularly regular aerobic exercise (which elevates brain estrogen-like compounds), Mediterranean diet adherence, quality sleep maintenance, and cardiovascular health optimization become even more critical for women carrying ε4.
Age as a Powerful Risk Modifier
Age dramatically influences when and whether ε4 genetic risk manifests as cognitive decline. In your 40s and early 50s, carrying ε4 poses no apparent cognitive threat—your brain shows no symptoms and cognitive testing appears normal. This "silent period" reflects preclinical Alzheimer's pathology developing without cognitive awareness.
Ages 60-75 represent the peak risk window when ε4 influence on cognitive decline becomes strongest. In this decade, genetic effects combine maximally with accumulated lifetime exposures (cardiovascular health, sleep quality, cognitive activity) to determine trajectories. After age 75, the influence of ε4 paradoxically diminishes: those who've avoided cognitive decline by 85 show lower subsequent dementia risk, suggesting protective factors have sufficiently offset genetic predisposition, or alternatively, only very robust individuals carrying ε4 survive to older age.
This age-dependent pattern has clinical implications: monitoring should intensify between ages 50-75 for ε4 carriers, while those beyond 85 without cognitive symptoms can usually cease intensive monitoring.
Ancestry and Genetic Diversity
Research consistently shows that APOE ε4 genetic risk varies across ancestral populations—a critical equity consideration often overlooked in genetic research. Populations of European ancestry show the highest Alzheimer's risk per ε4 allele. African ancestry populations show lower Alzheimer's risk despite ε4 carrier status, likely reflecting different genetic backgrounds and gene-environment interactions. Asian ancestry populations show intermediate risk patterns.
This variation means genetic counselors must interpret APOE results considering ancestral background. A ε4/ε4 individual of European descent faces substantially different risk than a ε4/ε4 individual of African descent. Additionally, most Alzheimer's genetic research has focused on European populations, creating equity issues: less is known about how other populations' genetic variants interact with ε4 to modify risk.
APOE Genotypes: Complete Guide to E2/E3/E4 Combinations
Your APOE genotype (the specific combination of two alleles you inherit) determines your genetic predisposition more precisely than any single SNP. Six possible combinations exist, each conferring distinct risk and protective profiles.
The Six APOE Genotypes Explained
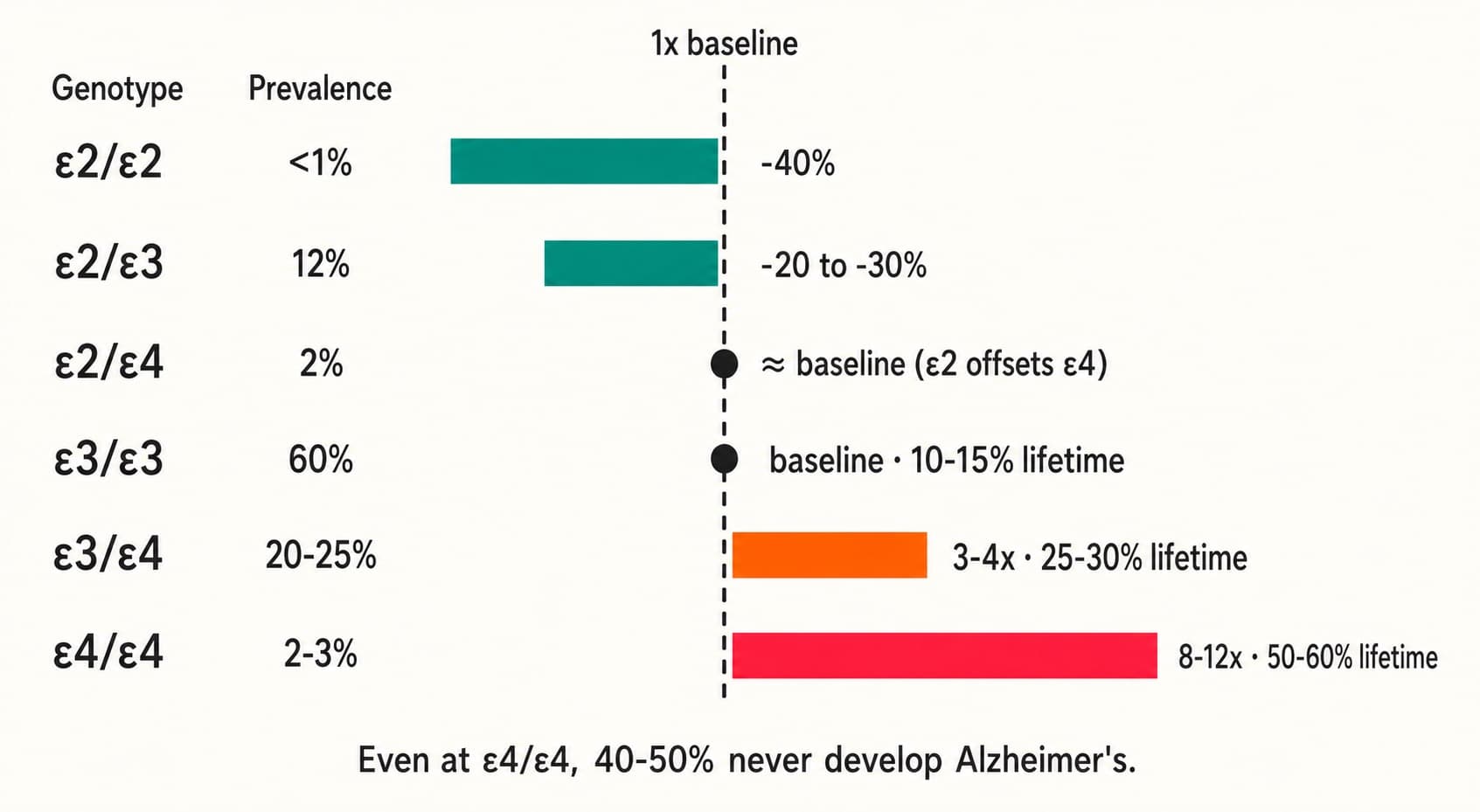
APOE ε2/ε2 (<1% of population) provides the strongest protection against Alzheimer's, reducing risk approximately 40% below the ε3/ε3 baseline. However, this genotype slightly increases risk for type III hyperlipoproteinemia—a lipid metabolism condition—creating a different health trade-off.
APOE ε2/ε3 (12% prevalence) confers mild protection, reducing Alzheimer's risk 20-30% compared to ε3/ε3. This genotype offers the most favorable combination for brain and cardiovascular health, explaining why some individuals live cognitively intact into their 90s.
APOE ε2/ε4 (2% prevalence) creates a genetic paradox: the protective ε2 allele partially counterbalances the risky ε4 allele, resulting in near-baseline Alzheimer's risk—nearly equivalent to ε3/ε3. These two alleles work in opposing directions regarding amyloid-beta clearance and neuroinflammation, creating relative equilibrium.
APOE ε3/ε3 (60% prevalence, the most common) represents the evolutionary neutral genotype, establishing baseline risk against which others are compared.
APOE ε3/ε4 (20-25% prevalence) shows the first substantial risk elevation—3-4 fold increase above baseline, with onset typically 5-10 years earlier than ε3/ε3 carriers.
APOE ε4/ε4 (2-3% prevalence) carries the highest risk: 8-12 fold increase with onset typically 10-15 years earlier than ε3/ε3.
The biological mechanism explaining these differences centers on amyloid-beta binding and clearance capacity. The ε2 allele binds amyloid-beta weakly, facilitating clearance and preventing plaque accumulation. The ε3 variant shows moderate binding affinity and moderate clearance. The ε4 allele binds amyloid-beta with high affinity but forms stable complexes resistant to clearance, promoting plaque accumulation.
Biomarker Progression: From Genetics to Pathology
Alzheimer's pathology progresses through distinct stages beginning at birth and extending decades before any cognitive symptoms appear.
Genetic risk stage (present from birth): Your rs429358 status is fixed, inherited from parents. Testing reveals this baseline.
Preclinical amyloid pathology stage (typically ages 40-50): PET imaging and cerebrospinal fluid testing reveal amyloid accumulation in the brain, yet cognitive testing remains normal and you notice no symptoms.
Preclinical cognitive changes stage (typically ages 50-60s): Advanced cognitive testing detects subtle decline imperceptible in daily life—processing speed slowing, memory pattern changes.
Mild cognitive impairment stage (typically ages 60-75): You notice memory or thinking problems affecting daily function, yet basic activities remain independent. Cognitive testing confirms decline.
Dementia stage (typically ages 70-85+): Cognitive decline progresses to interfering substantially with daily life, requiring assistance with activities.
For ε4 carriers, this timeline accelerates: stages compress by 5-15 years compared to ε3/ε3 carriers. Crucially, early intervention—when preclinical pathology exists but cognitive symptoms are absent—shows the greatest treatment efficacy. This is why biomarker monitoring matters: detecting pathology before symptoms enables maximum preventive impact.
Drug Response and Precision Medicine
Recent FDA-approved anti-amyloid monoclonal antibodies—drugs targeting and clearing brain amyloid directly—show promise particularly in ε4 carriers with early-stage disease. According to Cleveland Clinic research, APOE ε4 carriers often derive greater cognitive benefits from these medications compared to non-carriers. However, this comes with increased risk for amyloid-related imaging abnormalities (ARIA), particularly microhemorrhages visible on MRI.
Lecanemab (Leqembi) and donanemab represent the most advanced options, slowing cognitive decline by approximately 27-35% in early Alzheimer's disease when started in the preclinical or mild cognitive impairment stage. Traditional cholinesterase inhibitors show similar efficacy across all APOE genotypes, offering an alternative for those unable to tolerate newer anti-amyloid approaches.
The future of Alzheimer's treatment involves precision medicine incorporating APOE status into decision-making: genotype-informed dosing, predictive modeling of ARIA risk, and genotype-specific drug selection. Genetic counseling before treatment initiation becomes essential, ensuring informed consent regarding both benefits and risks specific to your genotype.
Prevention Strategies for APOE ε4 Carriers: Lifestyle and Medical Interventions
The central message for APOE ε4 carriers: genetic risk is not destiny. Evidence-based interventions can substantially reduce Alzheimer's risk, potentially offsetting the genetic increase. Research from the Alzheimer's Drug Discovery Foundation demonstrates that intensive lifestyle modification reduces cognitive decline risk 30-45% even in high-risk genotypes.
Exercise and Physical Activity
Physical activity stands as the single most powerful prevention strategy specifically for ε4 carriers. According to JAMA Neurology (2024), regular aerobic exercise—150+ minutes weekly—reduces Alzheimer's risk 45% in ε4 carriers, double the protective benefit in non-carriers.
The mechanisms are profound: exercise increases brain-derived neurotrophic factor (BDNF), enhancing neuroplasticity and synaptic formation. It improves cerebral blood flow, delivering more oxygen and nutrients to brain tissue. Exercise promotes hippocampal neurogenesis—literally creating new neurons in memory centers. Remarkably, aerobic activity directly reduces brain amyloid burden, as measured by PET imaging, suggesting exercise mobilizes amyloid clearance pathways.
Effective exercise for ε4 carriers combines aerobic intensity with consistency. Examples include brisk walking 45-60 minutes five times weekly, jogging 20-30 minutes three times weekly, cycling 45 minutes three times weekly, or high-intensity interval training (HIIT) 20 minutes three times weekly. Resistance training 2-3 times weekly adds additional benefits for muscle mass and metabolic health. The key is sustained moderate-to-vigorous intensity, not leisurely walking.
Early prevention proves critical: beginning intensive exercise in your 40s-50s establishes brain reserve that provides protection decades later. Those already experiencing cognitive decline show modest benefits, but prevention in asymptomatic individuals proves most effective.
Nutritional Approaches
Mediterranean and MIND (Mediterranean-DASH Intervention for Neurodegenerative Delay) diets reduce Alzheimer's risk 30-40% in large prospective studies. For ε4 carriers specifically, certain dietary components become especially critical.
Omega-3 fatty acids (DHA and EPA) deserve special emphasis: ε4 carriers metabolize these compounds less efficiently than non-carriers, requiring higher intake. Stanford research recommends 2-3 grams daily omega-3 for ε4 carriers versus 1-2 grams for non-carriers. Sources include fatty fish (salmon, mackerel, sardines), fish oil supplements, algae supplements, and plant sources (flaxseeds, walnuts).
Leafy greens—five or more servings weekly—provide folate, vitamins K and E, and polyphenols protecting against neuroinflammation. Berries three or more times weekly supply anthocyanins with strong anti-inflammatory and antioxidant properties. Whole grains provide B vitamins and fiber supporting healthy cholesterol and glucose metabolism. Limited saturated fat intake (less than 5% of calories) becomes more important for ε4 carriers, whose brains appear more sensitive to cholesterol-driven pathology.
Supplemental B vitamins (B6, B12, folate) show promise in preventing brain atrophy in ε4 carriers with elevated homocysteine levels. Curcumin (turmeric's active compound) demonstrates anti-inflammatory and anti-amyloid properties in laboratory studies, though human clinical trials remain limited. Phosphatidylserine may improve memory function in early cognitive decline.
A practical Mediterranean meal pattern: breakfast with whole grain toast, berries, and walnuts; lunch featuring leafy green salad with olive oil, legumes, and chickpeas; dinner combining fatty fish or poultry with roasted vegetables and whole grains. This pattern is not only effective but also economically accessible, challenging the misconception that healthy eating requires premium products.
Sleep Optimization and Glymphatic Health
APOE ε4 carriers show heightened sensitivity to sleep disruption—a critical vulnerability often overlooked. Quality sleep, particularly deep slow-wave sleep, activates the glymphatic system, your brain's nighttime cleaning mechanism that clears metabolic waste including amyloid-beta proteins. Disrupted sleep impairs this clearance, allowing waste accumulation.
Research demonstrates that consistent 7-8 hour sleep significantly lowers brain amyloid burden in ε4 carriers compared to shorter sleep. Sleep apnea—a breathing disorder causing repeated awakenings and oxygen dips—deserves particular attention in ε4 carriers. Untreated sleep apnea accelerates cognitive decline and amyloid accumulation. If you snore, experience daytime sleepiness, or have witnessed breathing pauses during sleep, sleep testing becomes important.
Sleep hygiene fundamentals for ε4 carriers include consistent sleep schedule (same bedtime and wake time even weekends), dark and cool sleeping environment (65-68°F), no screens one hour before bed, limiting caffeine after 2 PM, and regular exercise (but not within three hours of bedtime). If these basics don't produce 7-8 quality hours, medical consultation becomes warranted.
Cardiovascular Health as Brain Health
ε4 carriers show stronger associations between midlife cardiovascular risk factors (hypertension, high cholesterol, diabetes, smoking) and later Alzheimer's risk. The mechanism is straightforward: cardiovascular disease damages brain microvessels, disrupts the blood-brain barrier, and promotes inflammation throughout the brain.
Target values for ε4 carriers should be more aggressive than general population recommendations: blood pressure less than 120/80 mmHg, LDL cholesterol less than 100 mg/dL, fasting glucose less than 100 mg/dL, and BMI between 18-25. Annual cardiovascular screening—blood pressure, lipid panel, glucose testing—is prudent. Statin therapy appears particularly beneficial for ε4 carriers with elevated cholesterol, with evidence suggesting cognitive benefits beyond cardiovascular protection.
Smoking cessation is non-negotiable: smoking accelerates cognitive aging in ε4 carriers by 5-15 years compared to non-smokers. Diabetes management becomes especially critical, as diabetes-related metabolic changes synergize with ε4-related pathology to accelerate cognitive decline.
Cognitive Engagement and Cognitive Reserve
Your brain's cognitive reserve—the resilience allowing it to tolerate pathology without manifesting symptoms—builds through decades of challenging mental activity. ε4 carriers benefit especially from cognitive reserve, as pathology often develops despite maintained function.
Bilingualism shows the strongest evidence for cognitive reserve building. Multilingual individuals maintain cognitive function with greater amyloid pathology than monolingual peers, and they develop dementia 4-5 years later on average. Education and lifelong learning similarly build reserve: return to school, learn new languages, master instruments, engage with complex literature, pursue demanding work.
Social engagement is cognitive engagement: loneliness predicts cognitive decline, while active social networks protect cognition. Activities building reserve include chess, bridge, complex writing, artistic pursuits, and mentally demanding hobbies. Simple activities like television watching, even if complex shows, provide less reserve benefit than activities requiring active creation or problem-solving.
Cognitive engagement shows no age limit: older adults building cognitive reserve through learning show cognitive benefits within months. The principle "use it or lose it" holds: cognitive activity now protects your brain decades later.
Practical Implications: Living as an APOE ε4 Carrier
Genetic Testing Considerations
Testing for rs429358 makes sense if you have family history of Alzheimer's, are experiencing cognitive changes, or want objective risk assessment to guide prevention efforts. Your genetic counselor helps interpret results considering your ancestral background, family history, and personal circumstances.
Several testing approaches exist: rs429358-only testing (single SNP) provides basic information but less complete than full APOE genotyping (rs429358 plus rs7412, determining all six genotypes). Comprehensive Alzheimer's risk panels test APOE plus additional variants (CLU, BIN1, PICALM, APOB, MS4A4E, CD33) that also influence risk. Whole genome sequencing captures your complete genetic information, though requiring expert interpretation.
Direct-to-consumer genetic tests (23andMe, AncestryDNA, etc.) often include APOE information, generally accurate but best interpreted with professional genetic counseling rather than relying solely on company-provided risk estimates. Insurance coverage for clinical APOE testing varies; genetic counselors can guide you through coverage and cost considerations.
Understanding privacy implications matters: genetic data is sensitive information. The Genetic Information Nondiscrimination Act (GINA) in the United States prohibits health insurers from discriminating based on genetic information, but does not protect life insurance, long-term disability insurance, or employer-related concerns. Discuss privacy considerations with your healthcare provider before testing.
Psychological and Emotional Dimensions
Knowing you carry rs429358, especially if homozygous (ε4/ε4), naturally evokes anxiety. You're learning that your risk substantially exceeds population average. Importantly, this information carries psychological complexity worth acknowledging.
Some individuals find testing empowering: knowing enables action, building agency through prevention efforts. Others find knowledge anxiety-inducing without immediate plans to act. There's no "correct" response. Genetic counselors specialize in helping you process this information, discuss family implications, and decide whether testing aligns with your emotional readiness and action plans.
Support communities exist for ε4 carriers and families affected by Alzheimer's. Organizations like the Alzheimer's Association and Cognitive Vitality provide evidence-based education and peer support, helping reduce isolation and anxiety. Many ε4 carriers live cognitively intact into old age; centering this reality alongside honest risk discussion helps maintain psychological equilibrium.
Frequently Asked Questions
Q: What exactly is rs429358 and how does it differ from APOE genotype?
rs429358 is a single SNP (base pair variant) at one location within the APOE gene. This specific position determines whether you carry the ε4 allele. Your complete APOE genotype is determined by two SNPs: rs429358 and rs7412. Together, these two positions create one of six possible genotypes (ε2/ε2, ε2/ε3, ε2/ε4, ε3/ε3, ε3/ε4, ε4/ε4), each conferring different Alzheimer's risk. Knowing only rs429358 without rs7412 provides incomplete genotype information.
Q: If I carry one APOE ε4 allele (ε3/ε4), what's my actual Alzheimer's risk?
Your lifetime Alzheimer's risk approximately 25-30% if you carry one ε4 allele—roughly 3-4 times higher than the ε3/ε3 baseline of 10-15%. This means 70-75% lifetime probability of never developing Alzheimer's even with this genetic risk. Onset typically occurs 5-10 years earlier than in non-carriers if disease develops. However, these percentages represent population-level averages; your individual risk depends on other genetic variants, lifestyle factors, cardiovascular health, education, and cognitive activity. Prevention can substantially modify this trajectory.
Q: Can rs429358 predict when I'll develop Alzheimer's?
No. rs429358 provides risk probability but no predictive power regarding timing or certainty. Even individuals carrying two ε4 alleles—the highest-risk genotype—have 40-50% chance of never developing Alzheimer's. The variant indicates statistical risk elevation, not guaranteed disease development. Your actual risk depends on numerous modifiable factors: exercise, diet, sleep quality, cardiovascular health, cognitive engagement, education, and other genetic variants. This is why knowing your status becomes valuable: it prompts personalized prevention now, when prevention proves most effective.
Q: I carry ε4/ε4 (two copies). Does this guarantee I'll get Alzheimer's?
No. This is perhaps the most important message for those carrying two ε4 alleles. Despite 50-60% lifetime risk, roughly 40-50% of ε4/ε4 individuals never develop cognitive decline or dementia. Reaching age 85 without cognitive symptoms as an ε4/ε4 carrier suggests protective factors have sufficiently offset genetic predisposition. Intensive lifestyle modification (exercise, Mediterranean diet, quality sleep, cardiovascular optimization, cognitive engagement) can substantially reduce your actual risk, potentially offsetting the genetic increase. Knowledge of your status enables proactive, evidence-based prevention strategies that provide real protection.
Q: Does being female and carrying APOE ε4 increase my risk more?
Yes. Female APOE ε4 carriers show higher Alzheimer's risk compared to male carriers with identical genotypes. The protective effect of estrogen, naturally produced before menopause, decreases this risk in younger women. Post-menopausal women, lacking this estrogen protection, face acceleration of cognitive aging. This means female ε4 carriers require particularly aggressive prevention strategies: regular aerobic exercise (which elevates brain hormones mimicking estrogen effects), Mediterranean diet adherence, sleep optimization, and cardiovascular management become even more critical for women than for male counterparts with the same genotype.
Q: Are medications available specifically for APOE ε4 carriers?
Yes, recent anti-amyloid monoclonal antibodies show particular efficacy in ε4 carriers with early Alzheimer's disease. Lecanemab (Leqembi) and donanemab demonstrate greater cognitive benefits in ε4 carriers compared to non-carriers in clinical trials. However, ε4 carriers also experience higher rates of amyloid-related imaging abnormalities (ARIA), particularly microhemorrhages, requiring more intensive monitoring. Traditional cholinesterase inhibitors (donepezil, rivastigmine) show similar efficacy regardless of APOE status. Future precision medicine approaches will increasingly incorporate APOE genotype into treatment planning, dosing recommendations, and risk prediction before therapy initiation.
Q: What single intervention matters most if I carry rs429358?
Regular aerobic exercise—150+ minutes weekly at moderate-to-vigorous intensity—provides the most powerful single intervention for ε4 carriers, reducing Alzheimer's risk approximately 45% according to JAMA Neurology research. This exceeds benefits from any other single intervention. Mediterranean diet, quality sleep optimization, and cardiovascular health management follow as nearly equally important second-tier interventions. The evidence suggests that no single intervention provides complete protection; rather, combining multiple approaches multiplies protective benefits. Beginning intensive exercise, diet, and lifestyle optimization in your 40s-50s provides maximum protection.
Q: Can I completely prevent Alzheimer's if I'm an APOE ε4 carrier?
Not with 100% certainty—no prevention strategy guarantees disease avoidance. However, evidence demonstrates that intensive lifestyle modification can substantially reduce risk, potentially offsetting genetic increase. Large prospective studies show that individuals maintaining excellent exercise, diet, sleep, cognitive engagement, and cardiovascular health show dramatically lower dementia risk despite genetic predisposition. The key is early intervention: prevention strategies prove most effective before preclinical pathology begins, typically before age 50-55. Implementation of multiple interventions simultaneously produces synergistic protective effects exceeding any single approach.
Q: How should I interpret my genetic test result for rs429358?
Interpretation requires context that genetic counselors provide: your specific genotype (ε3/ε4, ε4/ε4, etc.), your ancestral background (which modifies risk interpretation), your family history, your personal medical history, and your individual health goals. The raw result—"T/T" or "heterozygous"—means little without this contextualization. A genetic counselor explains what percentage lifetime risk means, clarifies that probability is not certainty, discusses family implications (children's 50% inheritance per allele), and helps you decide whether increased monitoring, preventive strategies, or biomarker testing align with your preferences. Schedule genetic counseling before or shortly after testing to ensure proper interpretation.
Q: Are clinical trials available for APOE ε4 carriers specifically?
Yes. Multiple clinical trials currently recruit ε4 carriers to study prevention strategies, biomarker monitoring approaches, and new therapeutics. Trials testing lecanemab in preclinical stages specifically examine ε4-enriched populations, investigating whether earlier intervention in asymptomatic ε4 carriers provides greater benefit than standard clinical trials. Prevention trials examine whether anti-amyloid drugs or lifestyle interventions can prevent cognitive symptoms from ever developing. ClinicalTrials.gov (search "APOE" or "Alzheimer's prevention") lists ongoing opportunities. Ask My DNA provides resources connecting carriers with relevant trials matching their genotype and willingness to participate.
Q: Should I tell my family if I'm an APOE ε4 carrier?
This is a personal decision with no single correct answer. Genetic information affects relatives: children inherit 50% chance per ε4 allele you carry (100% if you're ε4/ε4). Some family members may find this information empowering, prompting early prevention. Others may experience unnecessary anxiety. Genetic counselors can help you navigate family disclosure, discussing both benefits (relatives can implement prevention) and potential psychological impacts. Some families benefit from family genetic counseling sessions where a counselor discusses implications for multiple relatives simultaneously. Your genetic information is your private health data; you control who learns about it.
Conclusion
Your rs429358 genetic status reveals important information about your Alzheimer's disease risk, but genetic predisposition never equals destiny. The APOE ε4 variant influences brain cholesterol metabolism, amyloid-beta clearance, and neuroinflammation in ways that increase risk, yet substantial evidence demonstrates that lifestyle modifications—intensive exercise, Mediterranean diet, quality sleep, cardiovascular optimization, and cognitive engagement—can substantially reduce this risk.
Research from Stanford, NIH, and major medical centers confirms that ε4 carriers implementing comprehensive prevention strategies during their 40s and 50s establish cognitive reserve that provides powerful protection decades later. Many individuals carrying two ε4 alleles live cognitively intact throughout their lives, suggesting that knowing your genetic status and acting on it provides real benefit.
If you carry rs429358, consider genetic counseling for personalized interpretation, discuss preventive strategies with your healthcare provider, and explore whether biomarker monitoring or clinical trial participation align with your health goals. Your genes establish baseline risk, but your daily choices—exercise today, healthy meals, quality sleep tonight, cognitive engagement—actively rewrite your Alzheimer's trajectory.
📋 Educational Content Disclaimer
This article provides educational information about genetic variants and is not intended as medical advice. Always consult qualified healthcare providers for personalized medical guidance. Genetic information should be interpreted alongside medical history and professional assessment.