rs1801133 is a common genetic variant—more than half of people in some ancestries carry at least one copy, and roughly 10-25% are TT homozygous depending on ancestry—yet most people have never heard of it. Also known as MTHFR C677T, this single nucleotide polymorphism reduces your MTHFR enzyme's efficiency by 30-70%, directly impacting how your body processes folate and regulates homocysteine levels. According to a 2024 Scientific Reports analysis, this variant explains significant inter-individual variation in homocysteine levels, making it one of the most clinically relevant genetic factors for cardiovascular health, mental well-being, and pregnancy outcomes.
Understanding your rs1801133 genotype is the first step toward optimizing your health. Whether you carry one copy (CT) or two copies (TT) of the C677T variant, research demonstrates that targeted nutritional strategies can dramatically improve your methylation capacity and reduce disease risk. This comprehensive guide provides everything you need to know about this common genetic variant and practical, evidence-based steps to manage it effectively.
Understanding rs1801133: The MTHFR C677T Variant
rs1801133, commonly known as MTHFR C677T, is a genetic variant where cytosine (C) is replaced by thymine (T) at position 677 of the MTHFR gene. This single nucleotide polymorphism reduces the enzyme's ability to convert folate into its active form by 30-70%, significantly impacting methylation capacity and homocysteine regulation.
What is rs1801133? Definition and Overview
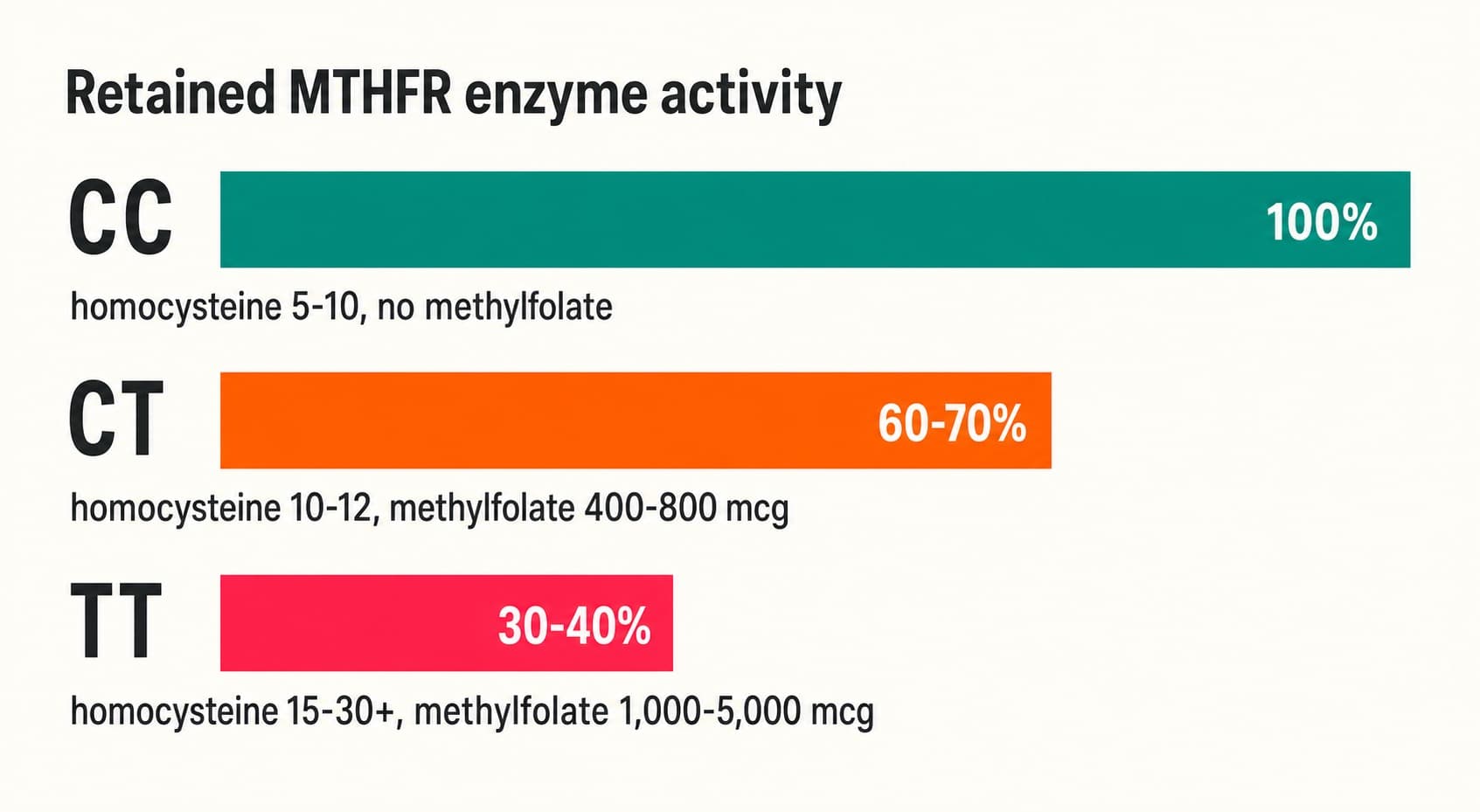
rs1801133 represents a cytosine-to-thymine substitution at codon 222 of the MTHFR (methylenetetrahydrofolate reductase) gene, resulting in an alanine-to-valine amino acid change. This variant creates what scientists call a "thermolabile" enzyme—one that is heat-sensitive and has reduced stability and activity compared to the normal form. The MTHFR enzyme catalyzes the conversion of 5,10-methylenetetrahydrofolate to 5-methyltetrahydrofolate (5-MTHF), the active form of folate required for critical methylation reactions throughout your body. According to research published in Nature Genetics (1995), individuals with one copy of the C677T variant (CT genotype) retain approximately 60-70% of normal MTHFR enzyme activity, while those with two copies (TT genotype) possess only 30-40% of normal activity levels. This enzyme impairment becomes particularly significant when dietary folate intake falls short of optimal levels, creating what researchers term a "functional folate deficiency."
Global Prevalence and Ethnic Variation
The rs1801133 variant demonstrates remarkable variation across different populations and geographic regions. Approximately 10-15% of individuals with Northern European ancestry carry the TT (homozygous) genotype, meaning they inherited the C677T variant from both parents. By contrast, Mediterranean and Hispanic populations show significantly higher prevalence rates, with 20-25% carrying the TT genotype. In the United States, estimates suggest that up to 40% of white Americans and Hispanic Americans carry at least one copy of the C677T variant. This ethnic variation likely reflects evolutionary adaptation to different dietary folate availability across regions and the relatively recent global food supply standardization. Geographic studies indicate that populations with traditionally lower dietary folate intake may have maintained higher frequencies of the C677T allele through natural selection, as the variant's effects remain minimal when folate intake is adequate.
The MTHFR Enzyme and Its Critical Role
The MTHFR enzyme occupies a pivotal position in your body's folate metabolism pathway. Dietary folate from leafy greens, legumes, and fortified grains undergoes sequential enzymatic conversions, ultimately producing 5-MTHF—the active form capable of accepting and donating methyl groups (CH₃) in methylation reactions. Once produced, 5-MTHF serves as the primary methyl donor for over 200 critical biochemical reactions in your body. These methylation reactions generate S-adenosylmethionine (SAM), often called the "universal methyl donor," which participates in DNA synthesis, neurotransmitter production, immune regulation, and homocysteine metabolism. When MTHFR enzyme activity is reduced by the C677T variant, folate accumulates in less active chemical forms, unable to undergo the final conversion to 5-MTHF. This bottleneck effect means that even individuals consuming adequate dietary folate may develop functional folate deficiency—their intake appears sufficient, yet their cells cannot access the active form required for methylation. Research demonstrates that this enzyme reduction is not theoretical; individuals with the TT genotype show measurably reduced methylation capacity in red blood cells, lymphocytes, and liver tissue when folate intake is marginal.
Understanding your MTHFR methylation genetics is the first step, but what truly matters is how rs1801133 impacts your unique genetic profile specifically. With Ask My DNA, you can explore your personal genetic data and discover exactly what this variant means for your methylation capacity and health trajectory.
How rs1801133 Affects Folate Metabolism and Methylation
The rs1801133 variant disrupts a fundamental biochemical process that your cells depend upon for survival and optimal function. To understand its effects, we must examine how folate metabolism normally operates and where the C677T variant creates a bottleneck.
The Folate Cycle and Methylation
The folate cycle represents one of your body's most critical metabolic processes, though few people understand its significance. Dietary folate from leafy vegetables, legumes, and fortified grains enters your digestive system and undergoes enzymatic processing. The MTHFR enzyme performs the final and rate-limiting step: converting 5,10-methylenetetrahydrofolate into 5-methyltetrahydrofolate (5-MTHF). This active folate (5-MTHF) then donates its methyl group to homocysteine, regenerating methionine (a step that also requires vitamin B12). Methionine is then activated to S-adenosylmethionine (SAM)—the universal methyl donor. SAM donates its methyl group to over 200 different substrates throughout your body: DNA bases (enabling DNA synthesis), phospholipids (essential for cell membranes), and proteins (modifying their function). After donating its methyl group, SAM becomes S-adenosylhomocysteine, which is hydrolyzed back to homocysteine. Homocysteine then has two fates: it can either be remethylated back to methionine (via the folate cycle) or converted to cysteine (via the transsulfuration pathway). This elegant cycle ensures that your body manufactures all the methylating power necessary for cellular function. However, according to research in the American Journal of Human Genetics (2002), individuals with reduced MTHFR activity experience impaired recycling through this cycle, leading to relative folate insufficiency and homocysteine accumulation.
Homocysteine and Cardiovascular Risk
Perhaps the most extensively studied consequence of rs1801133 is its effect on homocysteine metabolism. Homocysteine, a sulfur-containing amino acid, accumulates when the folate cycle cannot efficiently recycle it back to methionine. Elevated homocysteine initiates a cascade of harmful effects: it damages the endothelial cells lining your arteries through oxidative stress, promotes atherosclerotic plaque formation, increases blood clotting risk, and triggers chronic inflammation. Normal fasting homocysteine levels range from 5-10 μmol/L. The CDC reports that individuals with elevated homocysteine (above 15 μmol/L) face substantially increased cardiovascular disease risk. Specifically, meta-analyses published in JAMA (2002) found that each 5 μmol/L increase in homocysteine corresponds approximately to a 20% increase in coronary heart disease risk and a 10% increase in stroke risk. For individuals with the TT genotype of rs1801133, untreated homocysteine levels commonly reach 15-30 μmol/L or higher, translating to 2-3 times greater cardiovascular risk compared to CC genotype individuals with normal homocysteine (5-10 μmol/L). Importantly, this risk is not immutable. With appropriate methylfolate supplementation, B vitamin support, and dietary optimization, TT individuals can reduce homocysteine to healthy levels (below 10 μmol/L) and substantially mitigate cardiovascular risk.
Neurological and Mental Health Implications
The brain exhibits particularly high methylation demands due to its dependence on neurotransmitter synthesis, myelin production, and DNA repair processes. Research published in Translational Psychiatry (2018) reveals that individuals with the TT genotype of rs1801133 show altered brain methylation patterns compared to CC individuals. These methylation changes correlate with measurable neurological consequences. Depression risk increases approximately 1.4-fold in TT carriers compared to CC carriers. This connection likely operates through multiple mechanisms: reduced production of S-adenosylmethionine impairs synthesis of dopamine, serotonin, and norepinephrine—the neurotransmitters most critical for mood regulation. Additionally, impaired DNA methylation within brain cells may disrupt normal epigenetic regulation of genes involved in stress response and emotional processing. Some studies suggest cognitive differences, including challenges with processing speed and working memory, may occur more frequently in TT individuals with borderline folate status. Furthermore, the accumulation of homocysteine itself exerts neurotoxic effects, damaging cerebral blood vessels and promoting neuroinflammation. These findings don't indicate that rs1801133 TT individuals are destined for depression or cognitive decline. Rather, they demonstrate that optimal methylation support—achieved through adequate methylfolate, B vitamins, and dietary folate—becomes particularly important for neurological health in this genetic subgroup.
rs1801133 Genotypes: CC, CT, and TT Implications
Understanding the three possible rs1801133 genotypes—determined by whether you inherited zero, one, or two copies of the C677T variant—reveals how your genetic architecture influences methylation capacity and health outcomes.
The Three Genotypes Explained
The MTHFR C677T variant demonstrates simple Mendelian inheritance: you inherit one copy of the MTHFR gene from your mother and one from your father. If both parents contribute the normal C allele, you have the CC genotype. If one parent contributes C and the other contributes the T variant, you have the CT (heterozygous) genotype. If both parents contribute the T variant, you have the TT (homozygous) genotype. This genetic inheritance directly determines your MTHFR enzyme activity level. CC individuals possess two copies of the normal gene and therefore produce fully functional MTHFR enzyme at 100% activity levels. These individuals rarely experience folate metabolism problems unless other factors (severe dietary deficiency, malabsorption, medications interfering with folate) intervene. CT heterozygous individuals inherit one functional gene and one variant gene. Their MTHFR enzyme operates at reduced efficiency—approximately 60-70% of normal activity. While this reduction sounds substantial, most CT individuals maintain adequate methylation with normal dietary folate intake, particularly if they avoid significant stressors. TT homozygous individuals carry two copies of the C677T variant, resulting in severely compromised MTHFR enzyme function at only 30-40% of normal activity. This genetic status creates vulnerability to folate insufficiency and homocysteine elevation, particularly during periods of physiological stress (pregnancy, illness, excessive alcohol consumption) or inadequate folate intake.
Health Risks by Genotype
The health implications of each genotype vary substantially based on both genetic status and lifestyle factors, particularly dietary folate intake and B vitamin support. CC genotype individuals face baseline cardiovascular risk and require no special dietary intervention beyond the standard recommended folate intake of 400 mcg daily for adults. Their homocysteine levels typically remain in the normal 5-10 μmol/L range even when consuming typical American diets containing relatively modest folate. Depression risk, neural tube defect risk in offspring, and other folate-dependent health outcomes remain at population baseline for CC individuals.
CT heterozygous carriers occupy an intermediate position. With adequate dietary folate (600-800 mcg daily), most CT individuals maintain healthy homocysteine levels (10-12 μmol/L). However, CT carriers demonstrate vulnerability during specific circumstances: pregnancy substantially increases methylation demands, potentially pushing homocysteine toward 12-18 μmol/L; high alcohol consumption impairs folate absorption and increases homocysteine metabolism; certain medications (methotrexate, antiepileptic drugs, corticosteroids) further deplete folate; and high-stress periods increase methylation demands. A CT individual with excellent folate intake and low stress may experience better methylation markers than a CC individual consuming a folate-poor diet. This underscores a critical principle: genotype represents vulnerability, not destiny. Lifestyle and nutritional interventions can substantially influence health outcomes.
TT homozygous individuals face the most significant health challenges if methylation support remains inadequate. Untreated TT individuals commonly develop elevated homocysteine (15-30+ μmol/L), creating a 2-3 fold increase in cardiovascular disease risk, approximately 2-fold increased neural tube defect risk in offspring, increased depression risk (1.4-fold), and potential cognitive differences. Neural tube defects represent a particular concern: TT women of childbearing age planning pregnancy face substantially elevated risk of having children with spina bifida or anencephaly unless they receive aggressive methylfolate supplementation beginning 3-6 months before conception. According to research (2019), women with the TT genotype who experienced recurrent miscarriages benefited substantially from therapeutic intervention combining high-dose methylfolate with low-dose aspirin and enoxaparin. However, with appropriate methylfolate supplementation (1,000-5,000 mcg daily, titrated by homocysteine measurement), B vitamin support, and dietary optimization, TT individuals can achieve normal homocysteine levels and substantially mitigate disease risk.
Testing and Diagnosis Options
Determining your rs1801133 genotype requires genetic testing. The most accessible option involves accessing your raw DNA data from popular consumer genetic testing companies. Services like 23andMe and AncestryDNA test millions of SNPs including rs1801133; if you already have a 23andMe or AncestryDNA account, you can download your raw genetic data and upload it to free interpretation tools to learn your rs1801133 status. For those without existing genetic data, ordering direct-to-consumer genetic testing specifically for MTHFR variants (approximately $100-200) provides a straightforward approach.
Beyond genetic testing, functional assessment of your MTHFR status often provides more actionable information. Plasma homocysteine measurement reveals whether your actual methylation capacity is adequate. If you carry the TT or CT genotype but maintain homocysteine below 10 μmol/L with your current diet and lifestyle, your folate status is adequate. If homocysteine rises above 12 μmol/L, your methylation support is insufficient and requires intervention. The National Center for Biotechnology Information maintains ClinVar, a comprehensive database where you can search rs1801133 to access clinical significance data, prevalence information, and literature reviews supporting the variant's health implications.
If rs1801133 is part of your genetic profile, understanding your specific genotype reveals which methylation support strategies will most benefit you. Ask My DNA lets you discover your personalized methylation status, exploring how rs1801133 combines with other genetic variants like MTHFR A1298C, COMT, and MAO-A to determine your unique methylation requirements and optimal supplementation approach.
Managing MTHFR C677T: Methylfolate and Lifestyle Strategies
Effective rs1801133 management depends less on genetics alone and more on strategic nutritional optimization tailored to your specific genotype and homocysteine status.
Understanding Folic Acid vs Methylfolate: Myth Busting
One of the most widespread misconceptions about rs1801133 involves supplementation recommendations, particularly the notion that TT individuals must avoid folic acid entirely and instead take methylfolate exclusively. This myth has spawned thousands of social media posts and wellness advice suggesting folic acid is useless for C677T carriers. The CDC directly addresses this misconception in their guidance on MTHFR Gene Variants and Folic Acid: common MTHFR variants including C677T are not a reason to avoid folic acid. Contrary to the myth, folic acid does not depend on MTHFR to be absorbed: it is first reduced to active folate by a different enzyme, dihydrofolate reductase (DHFR), and MTHFR acts one step later on an intermediate that dietary folate passes through as well. Research shows folic acid raises blood folate and lowers homocysteine even in TT individuals—in one randomized trial, TT carriers on an adequate dose lowered homocysteine even more than CC carriers.
A major prospective study in ScienceDirect (published in American Journal of Clinical Nutrition) tracked folate metabolism in MTHFR C677T genotypes receiving standard folic acid supplementation. The research found that TT individuals receiving folic acid achieved folate levels only approximately 16% lower than CC individuals receiving the same folic acid dose—a modest difference that barely approached clinical significance. Furthermore, the CDC recommends that women who could become pregnant take 400 mcg of folic acid daily, regardless of MTHFR genotype. This evidence-based position reflects the scientific consensus that folic acid remains safe and reasonably effective even for TT carriers.
However, this doesn't mean methylfolate (5-MTHF) is irrelevant for C677T carriers. Methylfolate supplements provide folate already in the active form, completely bypassing the impaired MTHFR enzyme. For individuals with TT genotype and elevated homocysteine despite adequate folic acid intake, switching to methylfolate supplementation often proves more effective than folic acid. For most people, the choice between folic acid and methylfolate should be determined empirically: measure your homocysteine after 8-12 weeks using your current supplementation, and adjust based on results. If homocysteine normalizes with folic acid, continue it; if elevated homocysteine persists despite folic acid, transition to methylfolate.
Supplementation Strategies by Genotype
CC genotype individuals with adequate dietary folate require no supplementation beyond basic multivitamins containing standard folic acid. Consuming leafy greens, legumes, asparagus, and fortified grains typically provides sufficient folate.
CT heterozygous carriers should aim for 600-800 mcg of folate daily from dietary sources. Most achieve this through diet alone. During pregnancy, illness, or high stress, CT individuals benefit from 400-800 mcg supplemental methylfolate, which provides insurance against folate insufficiency. Many CT women planning pregnancy supplement with 800-1,000 mcg methylfolate daily throughout conception attempts and the first trimester.
TT homozygous individuals require more aggressive supplementation. Clinical experience and research support methylfolate supplementation of 1,000-5,000 mcg daily, titrated based on homocysteine measurement. Many practitioners recommend initiating at 1,000-2,000 mcg daily and increasing by 1,000 mcg increments every 4-6 weeks until homocysteine normalizes (target below 10 μmol/L). Some individuals achieve adequate homocysteine with 2,000 mcg, while others require 3,000-5,000 mcg daily.
Complete methylation support extends beyond folate alone. Vitamin B12 exists in multiple chemical forms; methylcobalamin (1,000-2,000 mcg daily) participates directly in homocysteine remethylation and proves more effective than cyanocobalamin for individuals requiring comprehensive methylation support. Vitamin B6 (pyridoxine, 25-50 mg daily) supports the transsulfuration pathway, an alternative route for homocysteine metabolism that reduces reliance on the folate cycle. Betaine (trimethylglycine, 500-2,000 mg daily) provides an entirely alternative remethylation pathway independent of MTHFR, donating a methyl group to homocysteine to regenerate methionine, effectively bypassing MTHFR enzyme limitation. For severe homocysteine elevation unresponsive to folate and B vitamins, betaine often produces dramatic improvements.
Dietary Optimization and Lifestyle
Dietary folate from fresh foods surpasses supplemental folate because whole foods contain folate alongside other nutritional cofactors supporting folate metabolism. Target 600-800 mcg daily from dietary sources for CT individuals and 800+ mcg for TT individuals. Excellent dietary sources include: cooked spinach (262 mcg per cup), cooked asparagus (262 mcg per cup), roasted Brussels sprouts (156 mcg per cup), cooked broccoli (78 mcg per cup), avocado (81 mcg per half), lentils (358 mcg per cooked cup), black beans (256 mcg per cooked cup), and chickpeas (282 mcg per cooked cup). Fresh vegetables contain superior folate content compared to frozen; frozen items retain most folate but cooked vegetables exceed raw in bioavailability due to heat-inactivated enzymes interfering with folate absorption.
Conversely, minimize synthetic folic acid from processed foods. Most processed foods contain folic acid added at fortification, not naturally occurring folate. While folic acid remains safe, individuals struggling to normalize homocysteine with current supplementation might benefit from emphasizing whole foods and methylfolate supplements rather than relying on folic acid from fortified foods and synthetic supplements.
Alcohol consumption substantially impairs folate metabolism and increases homocysteine. Individuals with CT or TT genotypes should minimize alcohol, particularly those with elevated homocysteine. Even moderate alcohol (1-2 drinks daily) can compromise methylation status in vulnerable individuals. For TT individuals with significant homocysteine elevation, temporary alcohol elimination may prove necessary until homocysteine normalizes.
Medications affecting folate warrant attention. Methotrexate, used for rheumatoid arthritis and certain cancers, directly depletes folate and necessitates supplementation. Antiepileptic medications (phenytoin, phenobarbital, valproate), oral contraceptives, and corticosteroids each deplete folate or increase homocysteine. If taking these medications, discuss specific supplementation requirements with your healthcare provider.
For women planning pregnancy with TT genotype, aggressive pre-conception intervention beginning 3-6 months before conception is essential. High-dose methylfolate (2,000-5,000 mcg daily), B12 supplementation, and B6 should begin immediately upon deciding to conceive, continuing throughout pregnancy. Homocysteine measurement should confirm adequate response; target levels below 10 μmol/L throughout pregnancy.
Special Considerations: Pregnancy and Mental Health
Certain life circumstances create particularly compelling reasons for TT individuals to optimize methylation support. Pregnancy and mental health represent two critical domains where adequate methylation provides tangible protection.
Pregnancy Planning for rs1801133 TT Carriers
Pregnancy represents the highest-risk circumstance for TT individuals with inadequate folate status. The developing fetus depends entirely on maternal methylation capacity for neural tube formation during gestational weeks 3-4. Neural tube defects—spina bifida and anencephaly—occur when neural tube closure fails due to insufficient methylation. TT women face approximately 2-fold increased neural tube defect risk compared to CC women with identical folate intake. This risk becomes catastrophic without intervention but becomes essentially equivalent to CC individuals with appropriate supplementation.
Evidence-based pregnancy planning for TT women requires: (1) Homocysteine measurement at baseline—target should be below 10 μmol/L before conception; (2) Initiating high-dose methylfolate (2,000-5,000 mcg daily) at least 3-6 months before attempting pregnancy, continuing throughout pregnancy and lactation; (3) Adding B12 and B6 supplementation; (4) Optimizing dietary folate; (5) Rechecking homocysteine at 4 weeks into supplementation and every 6-8 weeks throughout pregnancy; (6) Consulting both your OB/GYN and a practitioner experienced with MTHFR management before conception.
A landmark 2019 study in Fertility and Sterility examined 246 women with recurrent miscarriages (two or more consecutive pregnancy losses) who also carried the C677T variant. Researchers compared outcomes between women receiving standard prenatal care versus women receiving methylfolate (5,000 mcg daily), low-dose aspirin (81 mg daily), and enoxaparin (40 mg daily subcutaneously). The group receiving triple therapy achieved 70% live birth rate compared to only 20% in controls. While this study specifically examined miscarriage prevention rather than neural tube defect prevention, it demonstrates dramatic benefits of aggressive methylation support in TT pregnancies with adverse obstetric history.
Depression and Mental Health Support
The 1.4-fold increased depression risk in TT individuals, while notable, is not deterministic. Rather, it reflects increased vulnerability when methylation support becomes inadequate. Depression risk increases primarily among TT individuals with suboptimal folate status and elevated homocysteine. When methylation capacity is optimized through supplementation, depression risk approaches baseline.
Methylfolate specifically demonstrates augmentation effects in depression treatment. Multiple clinical trials show that adding methylfolate (5,000-15,000 mcg daily) to antidepressant medications improves treatment response compared to antidepressants alone. This mechanism likely operates through enhanced neurotransmitter synthesis: adequate 5-MTHF ensures sufficient SAM production for dopamine, serotonin, and norepinephrine methylation and synthesis. TT individuals experiencing depression should ensure comprehensive methylation support including adequate methylfolate, B12, B6, and dietary folate while working with psychiatrists or mental health providers. Some psychiatrists specialize in nutrigenomics and optimize methylation support as part of depression treatment protocols.
Frequently Asked Questions About rs1801133
Q: What does rs1801133 actually do to my body if I have it?
rs1801133 reduces your MTHFR enzyme activity by 30-70% depending on whether you carry one copy (CT) or two copies (TT) of the variant. This impairs your ability to convert dietary folate into 5-methyltetrahydrofolate, the active form required for methylation reactions. Reduced methylation capacity leads to elevated homocysteine, decreased neurotransmitter synthesis, impaired DNA methylation patterns, and increased disease risk for cardiovascular disease, neural tube defects, and depression. The severity of these effects depends on your genotype, dietary folate intake, B vitamin status, and lifestyle factors. With adequate supplementation and nutrition, TT individuals normalize homocysteine and substantially mitigate disease risk.
Q: Should I supplement with methylfolate if I have the rs1801133 C677T variant?
Supplementation depends on your specific genotype and current homocysteine level, not the variant alone. CC individuals rarely need methylfolate supplementation. CT individuals with adequate dietary folate (600-800 mcg daily) typically maintain healthy homocysteine without supplements, though many benefit from methylfolate during pregnancy or high-stress periods. TT individuals almost always benefit from methylfolate supplementation (1,000-5,000 mcg daily titrated by homocysteine measurement) to normalize homocysteine and optimize methylation. The best approach involves measuring plasma homocysteine: if it exceeds 12 μmol/L, supplementation is indicated; if it remains below 10 μmol/L, your current nutrition is adequate.
Q: Is rs1801133 TT genotype dangerous if left untreated?
Untreated TT genotype with elevated homocysteine (above 15 μmol/L) substantially increases cardiovascular disease risk (2-3 fold), neural tube defect risk in offspring (2-fold), and depression risk (1.4-fold). However, danger is contingent on untreated status and elevated homocysteine. TT individuals with adequate methylfolate supplementation, B vitamin support, and dietary optimization achieve normal homocysteine levels and normal disease risk. The variant itself isn't inherently dangerous; rather, it creates increased nutritional requirements. Meeting those requirements through supplementation and dietary optimization eliminates much of the excess risk.
Q: How does rs1801133 specifically affect my homocysteine levels?
The rs1801133 variant impairs conversion of dietary folate to 5-MTHF, the form required to remethylate homocysteine back to methionine via the folate cycle. With reduced MTHFR activity, this remethylation becomes bottlenecked, allowing homocysteine to accumulate. CC individuals typically maintain homocysteine 5-10 μmol/L. CT individuals commonly range 10-12 μmol/L and may rise to 12-18 μmol/L during stress or pregnancy. TT individuals frequently develop homocysteine 15-30+ μmol/L untreated. The relationship isn't purely genetic; a TT individual with excellent folate intake may achieve better homocysteine than a CC individual with poor nutrition. Homocysteine measurement determines whether your current folate status is adequate, regardless of genotype.
Q: Can I have a normal, healthy pregnancy if I have the rs1801133 TT genotype?
Absolutely yes, with appropriate management. TT women face 2-fold increased neural tube defect risk without intervention, but this risk becomes equivalent to CC individuals with adequate supplementation. Pre-conception methylfolate supplementation (2,000-5,000 mcg daily) beginning 3-6 months before conception, with homocysteine monitoring, reduces neural tube defect risk to baseline. Many TT women have healthy pregnancies with careful management. The key is beginning aggressive supplementation before conception, not waiting until after conception when neural tube formation is already underway.
Q: What is the actual difference between folic acid and methylfolate supplements?
Folic acid is synthetic folate requiring enzymatic conversion through your MTHFR enzyme (the step impaired by rs1801133) into 5-MTHF. Methylfolate (5-MTHF) is already the active form, completely bypassing MTHFR. For CC individuals, folic acid and methylfolate work equally well. For TT individuals with difficulty normalizing homocysteine on folic acid, switching to methylfolate often improves response. Both forms are safe; the choice should be empirically determined by measuring homocysteine on each supplementation form. The CDC confirms that folic acid remains effective even for TT carriers, though some individuals respond better to methylfolate.
Q: Do I need genetic testing for rs1801133, or is it just commercial hype?
Genetic testing for rs1801133 is genuinely valuable for individuals with relevant symptoms or risk factors: family history of early cardiovascular disease, elevated homocysteine, depression, recurrent miscarriages, neural tube defects in previous pregnancies, or planning pregnancy. Testing is not recommended for general screening in asymptomatic individuals per American College of Medical Genetics guidelines. If you have risk factors, testing clarifies whether rs1801133 contributes and guides supplementation decisions. If you already have 23andMe or AncestryDNA data, checking your rs1801133 status costs nothing—your raw data contains this information.
Q: What foods are highest in natural folate for rs1801133 carriers?
The highest-folate foods include: cooked spinach (262 mcg per cup), cooked asparagus (262 mcg per cup), roasted Brussels sprouts (156 mcg per cup), lentils (358 mcg per cooked cup), black beans (256 mcg per cooked cup), chickpeas (282 mcg per cooked cup), avocado (81 mcg per half), and cooked broccoli (78 mcg per cup). Fresh, minimally processed foods contain superior folate compared to processed items. Cooking actually increases folate bioavailability for some vegetables by inactivating enzymes that interfere with absorption. TT individuals should target 800+ mcg daily from diet, CT individuals 600-800 mcg daily, and CC individuals 400+ mcg daily.
Q: Can rs1801133 actually be treated or managed, or is it just genetic bad luck?
rs1801133 can be effectively managed through supplementation, dietary optimization, and lifestyle modification. It's not genetic "bad luck" requiring acceptance but rather a genetic variation creating increased nutritional requirements. Once you understand your genotype and homocysteine status, targeted interventions—methylfolate supplementation, B vitamins, dietary folate optimization, stress management, alcohol minimization—reliably normalize homocysteine and mitigate disease risk. Thousands of TT individuals successfully manage this variant through evidence-based strategies, achieving normal health outcomes indistinguishable from CC individuals.
Q: Does the rs1801133 TT genotype definitely cause depression?
No; TT genotype creates 1.4-fold increased depression risk, but depression is not inevitable. Most TT individuals never develop depression. Risk increases primarily in TT individuals with additional depression risk factors (family history, trauma, chronic stress, poor sleep) combined with inadequate methylation support (low folate, elevated homocysteine). TT individuals with excellent folate status and B vitamin support have depression rates approaching CC individuals. If you have TT genotype and depression, ensuring optimal methylation support is warranted, often in collaboration with psychiatrists experienced with nutrigenomics.
Q: What homocysteine level should I actually aim for as a therapeutic target?
Target plasma homocysteine below 10 μmol/L for optimal health. Most research shows cardiovascular disease risk increases substantially above 15 μmol/L, but optimal longevity and neural tube defect prevention occur when homocysteine remains below 10 μmol/L. Some practitioners target even lower levels (below 8 μmol/L) for patients with specific health conditions. Measure homocysteine every 6-12 months while adjusting supplementation to ensure you maintain healthy levels. If homocysteine rises above 12 μmol/L despite supplementation, increase methylfolate dose or evaluate other factors (B12 deficiency, certain medications, kidney disease) that may be elevating homocysteine.
Q: Should I take supplements if I have rs1801133 CT genotype?
CT heterozygotes don't uniformly require supplementation if maintaining adequate dietary folate (600-800 mcg daily). Homocysteine testing determines necessity: if your homocysteine is 8-10 μmol/L with current diet, supplementation isn't needed. If homocysteine rises above 12 μmol/L, supplementation is warranted. Additionally, CT individuals planning pregnancy, experiencing high stress, consuming high alcohol, or taking medications affecting folate should supplement preemptively. Methylfolate 400-1,000 mcg daily typically normalizes homocysteine in CT individuals requiring supplementation.
Conclusion
rs1801133 (MTHFR C677T) is a common genetic variant; more than half of people in some ancestries carry at least one copy, and roughly 10-25% are TT homozygous depending on ancestry. Rather than representing inevitable disease, it reflects an evolutionary variant creating increased folate and B vitamin requirements. Understanding your rs1801133 genotype—whether CC, CT, or TT—reveals your specific methylation vulnerabilities and informs targeted nutritional strategies. CT individuals with adequate dietary folate typically require no supplementation. TT individuals with elevated homocysteine benefit from folate supplementation (folic acid or methylfolate, 400-1,000 mcg daily), B12, B6, and dietary optimization. With appropriate management, TT individuals achieve normal homocysteine levels, normal cardiovascular risk, normal neural tube defect risk, and normal depression risk—indistinguishable from CC individuals. The key to successful rs1801133 management lies not in genetic fatalism but in empirical optimization: measure your homocysteine, implement targeted supplementation based on results, and reassess every 6-12 months. Consult with healthcare providers, genetic counselors, or practitioners experienced in nutrigenomics to optimize your personalized methylation support plan.
📋 Educational Content Disclaimer
This article provides educational information about genetic variants and is not intended as medical advice. Always consult qualified healthcare providers for personalized medical guidance. Genetic information should be interpreted alongside medical history and professional assessment.